This content was part of the Healthy People 2020 Law and Health Policy project, which ended in 2020.
Using Law and Policy to Promote Breastfeeding in the United States

More than 4 out of 5 women breastfeed their babies immediately after birth,1 but many encounter barriers that keep them from continuing to breastfeed despite health benefits for both mother and baby. Laws and policies can help communities increase breastfeeding rates. Laws and policies also supported the achievement of ambitious national goals proposed by Healthy People 2020.
This is a summary of the report, The Role of Law and Policy in Assisting Families to Reach Healthy People’s Maternal, Infant, and Child Health Breastfeeding Goals in the United States, which was the third in a series of reports that highlighted the practical application of law and policy to improve health across the nation. Each report also had success stories, or Bright Spots, that illustrated how communities had used law and policy to help meet their health goals and achieve Healthy People targets.
This report presented evidence-based policy solutions that community and tribal leaders, government officials, public health professionals, health care providers, lawyers, and social service providers could use in their own communities. Many of these policy solutions aligned with action steps identified in the 2011 resource The Surgeon General’s Call to Action to Support Breastfeeding.2
Download Fact Sheet [PDF - 1.73 MB]
Key Finding: Enhanced maternity care practices, provider training, access to supplies, and increased insurance coverage contribute to early adoption and continued breastfeeding
- To improve breastfeeding rates and help families reach their breastfeeding goals, the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) established the Baby Friendly Hospital Initiative (BFHI), which promotes evidence-based practices for breastfeeding success.3
- The BFHI established Ten Steps Care—10 specific steps that improve breastfeeding outcomes.4 Mothers who begin breastfeeding after giving birth in a Ten Steps hospital are more likely to keep breastfeeding through their child’s first birthday.5 These steps are now widely endorsed by maternal and child health authorities.
- Improving provider training is an important part of the Ten Steps. While many providers are knowledgeable about the health benefits of breastfeeding, many don’t feel they have enough training to help families who have trouble breastfeeding.6 Most providers are also influenced by their own experiences when counseling families.7 Organizations like the Centers for Disease Control and Prevention (CDC) and American Academy of Pediatrics (AAP) have developed effective training programs for providers. These programs address physician training objectives set by the Academy of Breastfeeding Medicine (ABM) and core competencies set by the United States Breastfeeding Committee (USBC).
- The Affordable Care Act requires most insurance plans to cover recommended breastfeeding support and supplies, like breast pumps, at no cost. Previously, these services often weren’t covered by private insurance, which created a barrier for families who couldn’t afford to pay out of pocket.
Key Finding: Family leave policies contribute to improved breastfeeding outcomes
- The federal Family and Medical Leave Act (FMLA) guarantees eligible employees up to 12 weeks of unpaid leave to care for a newborn and recover from pregnancy. Although evidence shows that more leave time is associated with better breastfeeding outcomes, 40% of the United States workforce is not eligible for FMLA, and many who are eligible can’t afford to take unpaid time off of work.8
- Mothers with longer maternity leaves are more likely to continue breastfeeding after they return to work outside the home, supporting the importance of family leave programs. However, only 15% of workers in the United States have access to paid family leave, and there are significant disparities among racial and ethnic groups.9,10
- As of December 2019, 9 states and the District of Columbia will guarantee paid family leave by 2022. These programs are linked to better breastfeeding outcomes. For example, California passed a paid leave law in 2004 which is associated with up to 20% increases in breastfeeding rates state-wide.11
- Many states also have regulations that support breastfeeding when mothers return to work after their leave ends. For example, Mississippi requires child care facilities to provide sanitary places for mothers to pump and store milk. Child care facilities in Maryland must train staff and have policies that promote breastfeeding. And Louisiana prohibits discrimination against breastfed babies in child care facilities.12
Key Finding: State implementation of federal assistance programs plays an important role in breastfeeding promotion
- Federal funding provides local health departments with support for breastfeeding initiatives. State and local health departments play an important role in providing breastfeeding support at the individual and community levels.
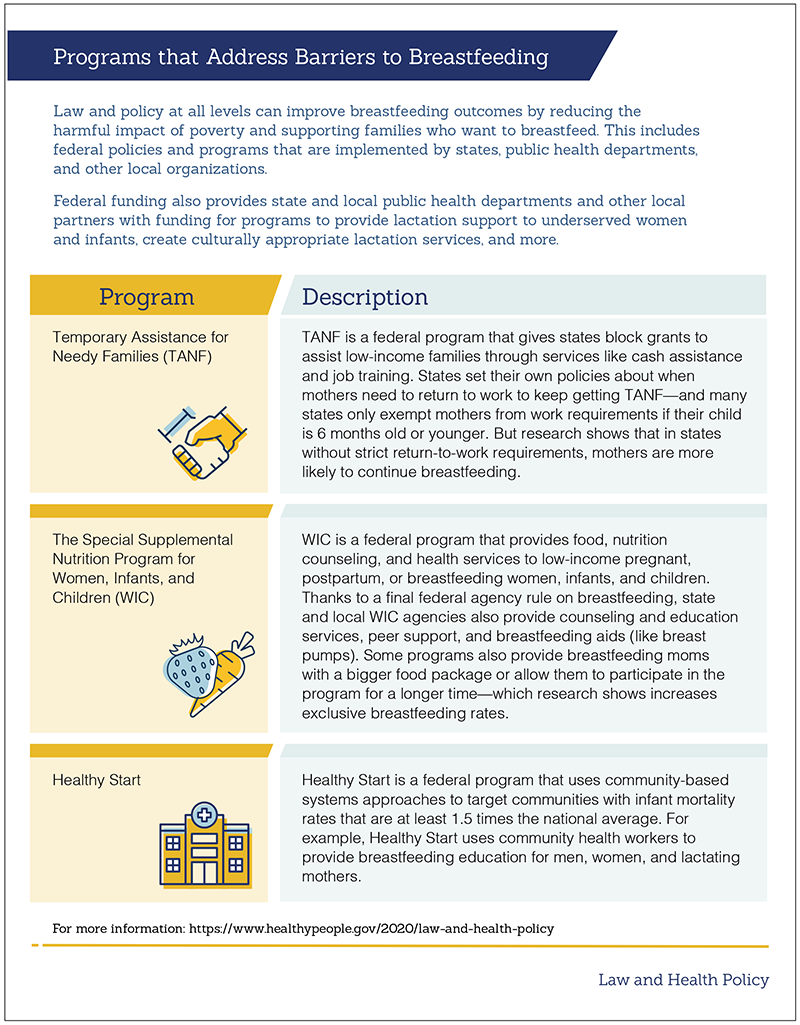
- Temporary Assistance for Needy Families (TANF) gives states block grants to assist low-income families through services like cash assistance and job training. Research shows that in states without strict return-to-work requirements for TANF for mothers with very young children, mothers are more likely to continue breastfeeding.
- The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) promotes breastfeeding in low income families by encouraging women to exclusively breastfeed and addressing common barriers faced by low income families. For example, women who are breastfeeding can participate in WIC for up to 1 year after birth—a longer time period than women who aren’t breastfeeding.
- Home visiting programs, like the Health Resources and Services Administration’s (HRSA) Maternal, Infant, and Early Childhood Home Visiting program (MIECHV), are associated with increased breastfeeding rates. Over 60% of MIECHV state grantees saw either increased breastfeeding initiation rates or increased breastfeeding duration rates.13
Featured Graphic: Programs that Address Barriers to Breastfeeding
Key Finding: Policies that support breastfeeding in places like workplaces, child care facilities, and public spaces encourage optimal breastfeeding practices
- Giving mothers a private, hygienic place to pump breastmilk at work benefits employers and employees. Mothers in supportive work environments are more productive and loyal to their company, and more likely to keep breastfeeding after they return to work.
- "Breastfeeding Friendly Worksite" programs recognize employers that support breastfeeding employees. To be recognized as breastfeeding friendly, employers may provide accommodations like flexible work schedules and the ability to safely and privately prepare, pump, and store breastmilk.
- Child care facilities can also be designated as "Breastfeeding Friendly" if they train staff to properly feed and store breastmilk, coordinate feeding times based on the baby’s normal feeding schedule, and provide families with written breastfeeding materials. Designating organizations also provide these child care facilities with support, resources, and technical assistance.
- State and federal policies protect the right to breastfeed in public places, although the level of protection—and enforcement—varies. All 50 states, the District of Columbia, the Virgin Islands, and Puerto Rico have laws allowing women to breastfeed in public. However, only 10 states, the District of Columbia, and Puerto Rico let breastfeeding mothers take legal action against those who have interfered with their right. Certain states also fine people who get in the way of someone’s right to breastfeed in public.
Featured Graphic: Breastfeeding Accommodations in Your Community
Key Finding: More research is needed to better understand the effectiveness of laws and policies that promote breastfeeding
- Although there are many evidence-based approaches to encourage breastfeeding, gaps in research make it difficult to assess the effectiveness of laws and policies that promote breastfeeding.
- Professionals can help build on existing evidence by improving data collection and standardizing data about infant feeding. This would make it easier to analyze the effect that changes in policy and practice have on breastfeeding outcomes.
- Continuing to investigate the impact of the Ten Steps on population health and health disparities would contribute to more robust evidence and support laws and policies that promote breastfeeding. Research on other support programs—like provider trainings, access to supplies, and paid family leave—could also inform and support beneficial laws and policies.
Conclusion
The Healthy People 2020 objectives related to improving breastfeeding practices in the United States are ambitious, but attainable. In fact, 3 of the targets have been met. To continue to improve and reach additional targets, federal, state, and local communities and organizations should leverage existing laws and policies.
To help the Nation meet health objectives related to breastfeeding, it’s important to:
- Continue to implement the BFHI and Ten Steps Care models
- Educate and train health care providers, child care workers, and employers about breastfeeding practice and promotion
- Encourage families to get the preventive care and breastfeeding supplies covered under the Affordable Care Act
- Evaluate the impact that paid and unpaid family leave has on families’ ability to reach breastfeeding goals
- Provide federal funding to state and local initiatives that promote breastfeeding
- Engage in further research to strengthen the relationship between breastfeeding law and policy and breastfeeding practice
Taking these steps will help ensure that families live in communities and environments that adequately promote and support breastfeeding, contributing to better health nationwide.
Related Healthy People 2020 Objectives
- MICH-21.1: Increase the proportion of infants who are ever breastfed
- MICH-21.2: Increase the proportion of infants who are breastfed at 6 months
- MICH-21.3: Increase the proportion of infants who are breastfed at 1 year
- MICH-21.4: Increase the proportion of infants who are breastfed exclusively through 3 months
- MICH-21.5: Increase the proportion of infants who are breastfed exclusively through 6 months
- MICH-22: Increase the proportion of employers that have worksite lactation support programs
- MICH-23: Reduce the proportion of breastfed newborns who receive formula supplementation within the first 2 days of life
- MICH-24: Increase the proportion of live births that occur in facilities that provide recommended care for lactating mothers and their babies
1. U.S. Department of Health and Human Services, Office of the Surgeon General. The Surgeon General’s call to action to support breastfeeding [Internet]. Washington (DC): 2011, cited 2019 Mar 20. Available from: https://www.ncbi.nlm.nih. gov/books/NBK52684/?report=reader.
2. U.S. Department of Health and Human Services, Office of the Surgeon General. The Surgeon General’s call to action to support breastfeeding [Internet]. Washington (DC): 2011, cited 2019 Mar 20. Available from: https://www.ncbi.nlm.nih. gov/books/NBK52684/?report=reader.
3. Bartick MC, Schwarz EB, Green BD, Jegier BJ, Reinhold AG, Golaizy TT, Bogen DL, Schaefer AJ, Stube AM. Suboptimal breastfeeding in the United States: maternal and pediatric outcomes and costs. Maternal & Child nutrition. 2017 Jan;13(1):e12366.
4. Baby-Friendly USA. The Baby-Friendly Hospital Initiative [Internet]. Albany (NY): Cited 2019 Mar 21. Available from: https://www.babyfriendlyusa.org/about/.
5. Feltner C, Weber RP, Stuebe A, Grodensky CA, Orr C, Viswanathan M. Breastfeeding programs and policies, breastfeeding uptake, and maternal health outcomes in developed countries. Comparative effectiveness review No. 210. (Prepared by the RTI International–University of North Carolina at Chapel Hill Evidence-based Practice Center under Contract No. 290-2015-00011-I.) AHRQ Publication No. 18-EHC014-EF. Rockville, MD: Agency for Healthcare Research and Quality; July 2018. Posted final reports are located on the Effective Health Care Program search page. DOI: https://doi.org/10.23970/AHRQEPCCER210.
6. Kramer MS, Chalmers B, Hodnett ED, et al. Promotion of Breastfeeding Intervention Trial (PROBIT): a Randomized Trial in the Republic of Belarus. JAMA. 2001;285:413-20.
7. Anchondo I, Berkeley L, Mulla ZD, et al. Pediatricians’, obstetricians’, gynecologists’, and family medicine physicians’ experiences with and attitudes about breast-feeding. South Med J. 2012;105:243-8.
8. Glynn SJ, Farrell J. Latinos least likely to have paid leave or workplace flexibility [Internet]. Washington, DC: Center for American Progress; 2012 Nov 20, cited 2019 Mar 25. Available from: https://www.americanprogress.org/issues/ economy/reports/2012/11/20/45394/latinos-least-likely-to-have-paid-leave-or-workplace-flexibility/.
9. Dixit A, Feldman-Winter L, Szucs KA. “Frustrated,” “Depressed,” and “Devastated” pediatric trainees: U.S. academic medical centers fail to provide adequate workplace breastfeeding support. J Hum Lact. 2015.
10. U.S. Department of Labor, Bureau of Labor Statistics. Employee benefits in the United States National Compensation Survey: employee benefits in the United States, March 2017 (Tables 16 and 32) [Internet]. Washington (DC): 2017 Sept, cited 2017 October 16. Available from: https://www.bls.gov/ncs/ebs/benefits/2017/ebbl0061.pdf.
11. National Partnership for Women and Families. Updating the Family Medical Leave Act [Internet]. Washington (DC): 2016 Jun, cited 2019 Mar 25. Available from: http://www.nationalpartnership.org/research-library/work-family/fmla/ updating-the-fmla.pdf.
12. Huang R, Yang M. Paid maternity leave and breastfeeding practice before and after California’s implementation of the nation’s first paid family leave program. Econ & Human Bio. 2015 Jan 31;16:45-59.
13. U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal Child Health Bureau; in collaboration with the Administration on Children and Families. Demonstrating improvement in the Maternal, Infant, and Early Childhood Home Visiting Program: a report to Congress. Washington (DC): 2016 Mar, cited 2019
Mar 26. Available from: https://mchb.hrsa.gov/sites/default/files/mchb/MaternalChildHealthInitiatives/HomeVisiting/pdf/reportcongress-homevisiting.pdf.