
Innovative Structure
Adapts existing infrastructure to create the nation’s first statewide health and human services care coordination platform, an innovation that facilitates collaboration and has enabled rapid scaling and delivery of evidence-based interventions for health-related social needs.
Whole-person Health
Establishes closer links between the health and human services sectors to better address social needs that impact health care costs and health outcomes, including by leveraging state Medicaid dollars to pay for services in domains such as food, housing, and transportation.
Local Investment
Recognizes the critical role of community-based organizations in furthering local uptake and invests in upfront capacity building to expand the ability of local organizations to provide reimbursable services to community members.
Bright Spot Profile
The North Carolina Department of Health and Human Services (NC DHHS) is a government entity that helps to advance Food Is Medicine (FIM) efforts through its Healthy Opportunities Pilot (HOP) program.
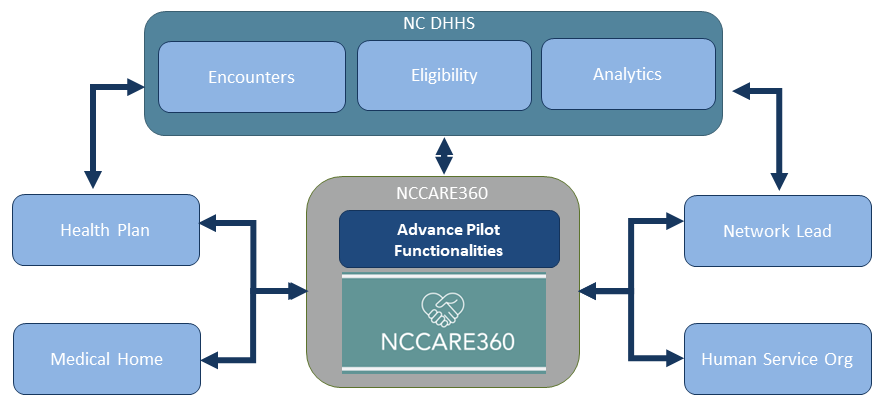
Key to NC DHHS’s success are the partnerships it has leveraged with Health Plans, regional care hubs called “Network Leads”, and community-based organizations (CBOs). Through a no-wrong door approach, care management teams refer beneficiaries for services using NC DHHS’s existing statewide health care technology platform (NCCARE360).
NC DHHS is featured in the Bright Spot series as an exemplar of state agencies creating systemic FIM approaches.
Notably, HOP is the nation’s first comprehensive program to test and evaluate the impact of providing select evidence-based, non-medical interventions related to housing, food, transportation, and interpersonal safety and toxic stress to high-needs Medicaid enrollees. (North Carolina Department of Health and Human Services, 2024)
This Bright Spot serves as a model to other FIM implementers on how they can leverage partnerships with CBOs to identify community-specific needs and increase participation in their FIM programs.
Healthy Opportunities
Impetus for Establishing Healthy Opportunities Pilot
Research has shown that 80 percent of health outcomes are driven by factors outside of clinical care settings (Magnan, 2017); however, health dollars have traditionally been spent exclusively on clinical care.
To address this discrepancy, NC DHHS developed a series of initiatives and a statewide infrastructure to connect health and human services and address whole person needs. It leveraged this existing infrastructure to implement the HOP program. Through HOP, North Carolina uses Medicaid dollars to pay for services that address individuals’ health-related social needs (HRSN) — such as improving access to food, housing, and transportation and promoting interpersonal safety — with the goal of improving health outcomes, reducing social need, and decreasing health care costs.
HOP Implementation Framework
NC DHHS began designing and implementing the Healthy Opportunities portfolio in 2017, including design of HOP as a Medicaid 1115 demonstration pilot which was approved by the Centers for Medicare and Medicaid Services (CMS) in 2018 for a demonstration period from 2019 to 2024.
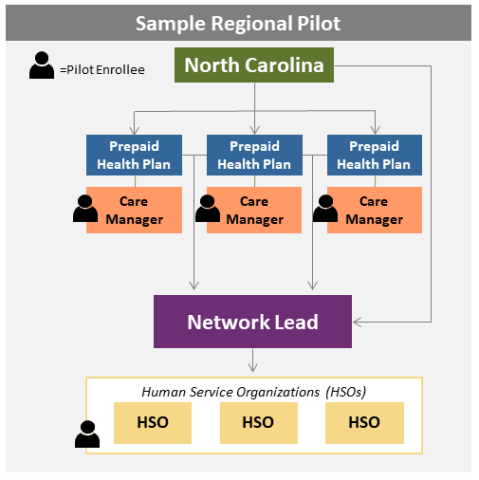
Through a request for proposal, HOP competitively procured three Network Leads entities to develop and oversee a network of CBOs, referred to as Human Services Organizations or HSOs, that provide 28 federally approved HOP services. The Network Leads were chosen based on their proposed ability to fulfill the requirements of HOP and geographic spread across the state.
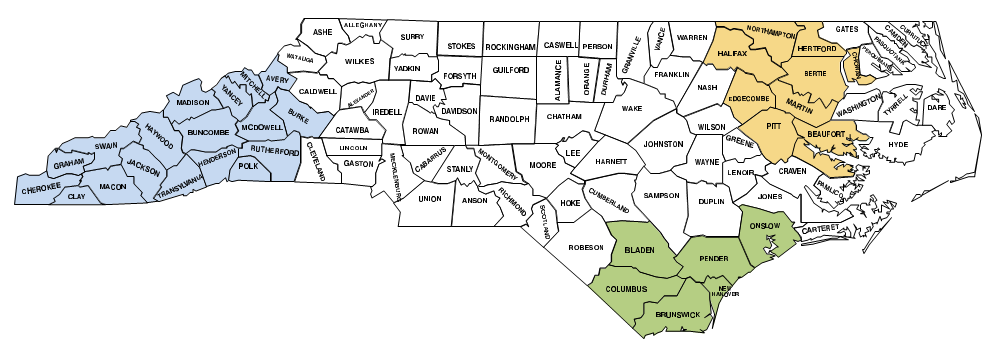
The Network Leads — Access East, Inc., Community Care of the Lower Cape Fear, and Impact Health — each identified their own catchment area and provide three regions of North Carolina with access to HOP services, consisting of 33 predominantly rural counties with diverse populations.
In addition to building out the network of providers, Network Leads provide technical assistance and training for the HSOs, such as how to bill for services and meet the program’s contractual requirements. The Network Lead approach was taken to create a bridge between the Managed Care Plans and the HSOs to build the capacity for cross-sector collaboration.
HOP participants are Medicaid beneficiaries who meet the program’s eligibility criteria and live in one of the 33 counties covered by the Network Leads. To meet eligibility criteria for HOP, participants must have at least one physical or behavioral health risk factor and one social risk factor.
HOP Outcomes
As of June 2024, over 20,000 North Carolinians have used HOP services and more than 455,000 services have been delivered by 147 CBOs, at a monthly health care cost savings of $85 per participant. Food services are the most common service type, representing about 85 percent of all services delivered. The Interim Evaluation Report states that HOP has resulted in the following benefits:
- Reduced emergency department use
- Reduced inpatient hospitalizations for non-pregnant adults by two admissions per month per 1,000 beneficiaries
- Reduction in the total number of social needs and services used across housing, food, and transportation domains
- Greater reductions in direct service spending observed in those who participated in HOP for longer periods of time
- Longer utilization of services linked to greater improvement
HOP Infrastructure
Statewide Infrastructure
NC DHHS built a statewide infrastructure that aimed to provide shared assets that could be used in all populations and Medicaid managed care plans. This infrastructure was leveraged and modified to create HOP. To build this infrastructure, NC DHHS developed a technical advisory group of health and human services providers to standardize a set of social needs screening questions that could be used by providers for all populations and would be contractually required for Medicaid managed care plans. The Network Leads create contracts with human service organizations whose services are accessible to beneficiaries served by all participating Health Plans. Additionally, NC DHHS built upon its existing medical home model to establish a strong network of primary care practices providing delegated care management services who also refer qualifying beneficiaries into HOP.
NCCARE360
Through a public-private partnership, the private, non-profit Foundation for Health Leadership & Innovation issued a request for proposals to find a vendor for a technology platform known as NCCARE360, which serves as a statewide closed-loop referral system that can be used for all populations and connects North Carolinians with the community resources required to meet their social needs.
NC DHHS works closely with the vendor to develop advanced technology to meet the authorization, billing and communication functionality needed to effectuate HOP service delivery.
Obtaining Stakeholder Feedback
Throughout the HOP design process, NC DHHS continued to convene stakeholder meetings and identify the best methods to use when implementing HOP. This process included leveraging the Commonwealth Fund to convene stakeholders and develop the fee schedule. NC DHHS also issued a request for information, intended for stakeholders who were unable to attend in-person meetings. NC DHHS used a phase-in approach for HOP service delivery.
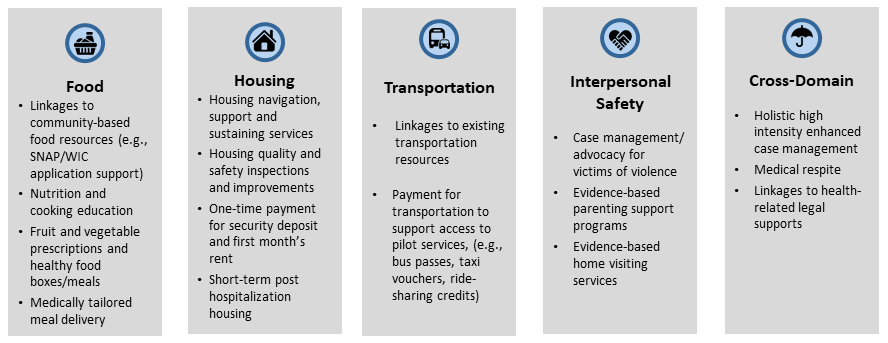
The phase-in approach indicated that food, housing, transportation, toxic stress, and sensitive (e.g., interpersonal violence) services would become available across all participating regions at different times; services in the food domain were the first available. Advanced functionalities specific to HOP requirements were built upon the existing statewide NCCARE360 platform.
Medicaid 1115 Demonstration
In 2017, NC DHHS began designing its 1115 demonstration which served as the vehicle for moving to Medicaid Managed Care in NC and also authorized North Carolina Medicaid to implement HOP. North Carolina is renewing its 1115 demonstration, which, once approved, will begin its second HOP demonstration period in November 2024.
Obtaining Stakeholder Feedback
Throughout the HOP design process, NC DHHS continued to convene stakeholder meetings and identify the best methods to use when implementing HOP. This process included leveraging the Commonwealth Fund to convene stakeholders and develop the fee schedule. NC DHHS also issued a request for information directed at stakeholders who were unable to attend in-person meetings.
NC DHHS used a phase-in approach for HOP service delivery. The phase-in approach indicated that food, housing, transportation, toxic stress, and sensitive (e.g., interpersonal violence) services would become available across all participating regions at different times; services in the food domain were the first available.
HOP Infrastructure Funding Sources
NC DHHS leveraged funding from a variety of sources to build the statewide infrastructure to implement HOP.
Below are the major milestones in NC DHHS’s journey to funding HOP:
- NCCARE360 was primarily funded through private philanthropic dollars in the first few years of implementation
- During the pandemic when health-related social needs rose, NC DHHS leveraged the Coronavirus Relief Fund (U.S. Department of Treasury, 2024) to provide funding to Foundation for Health Leadership and Innovation to expand the NCCARE360 system and support social service pilots
- NC DHHS was also able to leverage funding from federal grants, including the CDC Health Disparities Grant, to increase the capacity of CBOs to use NCCARE360 and deliver social services
- Through Medicaid Managed Care, NC DHHS developed financial levers for Managed Care Plans to be able to invest in social needs. These include allowing social services to be included in managed care capitation rates as value-added services, in lieu of services, and as clinical services.
- HOP-specific services and capacity building are supported by funding authority from the 1115 Medicaid demonstration pilot. The 1115 demonstration permitted a capacity building period for HOP so that participating CBOs would have time to receive funding from NC DHHS, hire qualified personnel, and train staff to provide HOP services.
Local Partnerships
Through the Network Leads, NC DHHS partners with CBOs such as food banks, food pantries, legal services organizations, housing agencies, transportation providers, and churches to leverage CBO knowledge of community-specific needs while providing financial support in their overall strategy to address social needs and deliver HOP services. NC DHHS identified application criteria, and each Network Lead developed an application and assessment using those criteria and contracted with CBOs in its respective region.
Throughout the HOP design and implementation processes, NC DHHS leveraged the Network Lead entities to partner with and convene local grassroots organizations to obtain feedback and make modifications to the HOP model based on CBO input. Partnerships with CBOs and local grassroots organizations have allowed NC DHHS to invest in local capacity and create a program that is rooted in local communities.
Reduce Health Disparities
The primary reason NC DHHS developed its strategy to address health-related social needs was to reduce health disparities statewide. To promote equity within HOP, NC DHHS ensured that the governing bodies of the Network Leads responsible for onboarding CBOs were representative of the populations that would be served in their region.
This approach leveraged the strength and insight of people with lived experience that could inform the effective design, implementation, and delivery of services for communities in which they live. NC DHHS also directed their Medicaid managed care plans to prioritize high-need populations when promoting enrollment in HOP.
Key Components to Success
Statewide Infrastructure
NC DHHS attributes its success in addressing health-related social needs and developing and implementing HOP to the creation and accessibility of a statewide multi-component shared infrastructure, commitment to investing in local communities, continuous communication with partners, attention to detail, creativity, and humility.
The statewide multi-component infrastructure facilitates the sharing of assets and tailored initiatives that can be used to build the evidence base and bridge health care and human services across diverse populations and geographies. Access to this infrastructure was essential for NC DHHS because it facilitated the rapid scaling and delivery of HOP.
Connecting with Care Management
NC DHHS Medicaid beneficiaries have access to care management to support their medical and non-medical needs through their Health Plan partners and community-based delegated care management entities. These entities screen for HOP social needs, and supporting beneficiaries with access to CBO services through the HOP referrals strengthens the relationships and trust between care managers and the beneficiaries they serve. Thus, when beneficiaries have other medical needs for which they need help navigating access or managing their care, they have a care management team who is available and trusted.
Investing in Local Communities
Choosing to invest in local communities helped NC DHHS leverage the expertise in communities, ensure the sustainability of HOP, and invest in the economic growth of communities. FIM is an important framework for HOP services and helps North Carolina establish relationships with local care teams.
For example, food services are the most common services delivered under HOP. The delivery of food services, especially at the community level, creates the opportunity for relationship building and more holistic care. The intentional “inefficiency” of in-person food delivery builds trust and connection, which then facilities people’s engagement in broader care teams and the identification and addressing of other unmet needs.
NC DHHS developed operational focused meetings with their local partner networks, which allowed for rapid identification and resolution of problems with HOP service delivery.
Lessons Learned
Investing in CBOs
Investing in locally based CBOs to deliver HOP services provided a key pathway to success because CBOs can leverage their connections with community members to encourage participation. To establish CBO capacity for service provision, NC DHHS utilized Network Leads to establish the regional relationships and leveraged the 1115 demonstration to allow for upfront capacity building dollars through Medicaid prior to service delivery. This was an essential task because most CBOs are under resourced, resulting in an inability to readily provide HOP services up front and then seek reimbursement from payors later.
Longer Time Horizons
While implementing HOP, NC DHHS learned that food facilitates human connections, addresses social isolation, and helps to build a sense of community. Access to food services also tended to increase trust and create a relationship through which beneficiaries later shared other social or medical needs.
Participants who received HOP services for longer periods saw greater reduction in health-related social needs and health care costs than those who were enrolled in HOP for a short time.
References
- North Carolina Department of Health and Human Services, 2024. Healthy Opportunity Pilots. https://www.ncdhhs.gov/about/department-initiatives/healthy-opportunities/healthy-opportunities-pilots
- Magnan, 2017. Social Determinants of Health 101 for Health Care. National Academy of Medicine Perspectives. https://nam.edu/wp-content/uploads/2017/10/Social-Determinants-of-Health-101.pdf
- U.S. Department of the Treasury, 2024. Coronavirus Relief Fund. https://home.treasury.gov/policy-issues/coronavirus/assistance-for-state-local-and-tribal-governments/coronavirus-relief-fund